
 English
EnglishThe Third Engineer (3/E) on board an anchored capesize bulk carrier was splashed by hot sludge while opening the manhole cover of a settling tank and subsequently died from a septic shock having sustained 2nd degree burns to a large part of his body
WHAT HAPPENED?
The Third Engineer (3/E) on board an anchored capesize bulk carrier was splashed by hot sludge while opening the manhole cover of a settling tank and subsequently died from a septic shock having sustained 2nd degree burns to a large part of his body.
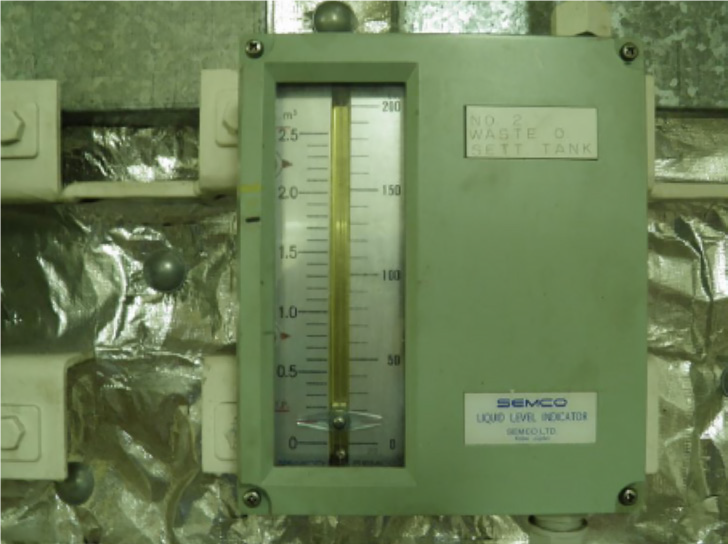
A quantity of sludge had been transferred from the “Bilge Separator Oil Tank” (BSO Tank) to No.2 “Waste Oil Settling Tank” (No.2 WOS Tank) using the sludge pump. However, it was observed that the level gauge of No.2 WOS Tank (Figure 1) was not indicating the correct quantity and it was subsequently confirmed that the gauge had malfunctioned.
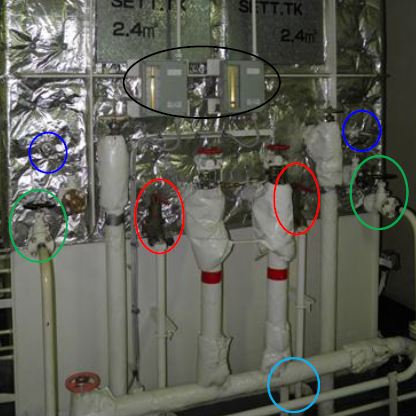
A “Job Hazard Analysis” (JHA) was therefore prepared and the Second Engineer (2/E), was assigned to drain the sludge residues from No.2 WOS Tank, which was situated adjacent to No.1 WOS Tank (Figure 2) and repair the gauge assisted by the 3/E.
The 2/E opened the valve to drain the sludge to the BSO Tank by gravity. In order to confirm that the tank was empty, the 3/E climbed on top and turned the scale reduction device wheel and reported it working. The 2/E noted a small movement of the level indicator while the valve was open. Finally, the 2/E opened the self-closing drain valve and a small quantity of water flowed through, then stopped.
The 2/E was therefore convinced that the tank was empty and the 3/E proceeded to open the manhole (Figure 3), about two metres above the floorplates. He removed all of the nuts from the cover apart from four, which he loosened.
AS HE DID NOT OBSERVE ANY LEAKAGE, HE THEN PULLED THE COVER WITHOUT REMOVING THE NUTS. HOWEVER, HOT OIL SPLASHED FROM THE MANHOLE BOTTOM ONTO THE 3/E, WHO WAS STANDING ON A FOLDING LADDER.
The 2/E pulled the 3/E away and took off his coveralls which were soaked with the oil. The 3/E was taken to the ship’s hospital where it was observed that he had sustained serious burns. The Chief Officer (C/O) provided the 3/E with first aid and a helicopter arrived about two hours after the accident and transferred him to a shoreside hospital, where he tragically died 12 days later.

Further details about the incident and the lessons learned are provided in the summary of the case study.
In addition, a presentation and reflective learning form have been prepared based on the incident as suggested training materials. These can be used by Members or their crew in any way they see fit to encourage reflection and gain the maximum learning from this incident: to consider why the incident happened; “what it means to me”, and to then relate the identified learning points to one’s own personal situation.
Finally, a Britannia commentary on the incident has been prepared which discusses the key points in more detail in order to help develop the reflective learning from the case study.
CASE STUDY MATERIAL
BSAFE INCIDENT CASE STUDY NO.1 – SUMMARY
BSAFE INCIDENT CASE STUDY NO.1 – REFLECTIVE LEARNING FORM
Summary of Lessons Learned
The following lessons learned have been identified based on the available information in the investigation report and are not intended to apportion blame on the individuals or company involved:
- The investigation found that the potential hazards related to the unknown quantity of hot sludge remaining in the tank due to the malfunctioning level gauge had not been identified.
- Making assumptions about the safety of the work environment can lead to unexpected hazard exposure and injury.
- It is possible that confirmation bias (favouring information that confirms one’s previously existing beliefs) led to the engineers being convinced that the tank was empty.
- Taking shortcuts from an established safe work procedure to save time and effort may be appealing, but can lead to undesirable and even tragic consequences.
- The vessel’s Planned Maintenance System (PMS) did not address the preventable jamming of the gauges with sludge by providing guidelines for periodic routine maintenance/tank cleaning.
- The WOS Tank was not fitted with a sounding pipe as an alternative means of verifying the contents of the tank when the level gauge malfunctioned.
- The 3/E was wearing a cotton coverall provided by the company; this would have only provided limited protection from heat and would have allowed penetration of the hot liquid.
This case study is drawn from the investigation report 14/2013 published by the Hellenic Bureau for Marine Casualties Investigation – HBMCI.
The purpose of this case study is to support and encourage reflective learning. The details of the case study may be based on, but not necessarily identical to, facts relating to an actual incident. Any lessons learned or comments are not intended to apportion blame on the individuals or company involved. Any suggested practices may not necessarily be the only way of addressing the lessons learned, and should always be subject to the requirements of any applicable international or national regulations, as well as a company’s own procedures and policies.