
 English
EnglishA CREW MEMBER SUFFERED A FATAL HEAD INJURY ON BOARD A 20,236GT GENERAL CARGO VESSEL WHICH WAS IN THE PROCESS OF LOADING GRAIN WHILE MOORED ALONGSIDE ANOTHER BULK CARRIER. THE CREW MEMBER WAS UNEXPECTEDLY STRUCK BY A TENSIONED MOORING LINE WHICH WAS BEING USED TO PULL THE VESSEL FORWARD DURING A WARPING OPERATION, BUT UNFORTUNATELY SPRANG LOOSE FROM THE FAIRLEAD, RESULTING IN THE TRAGIC ACCIDENT.

Source Fleetmon
WHAT HAPPENED
The incident occurred between two bulk carriers, while anchored. Vessel A arrived at the anchorage to load grain from another anchored bulk carrier (vessel B). A pilot boarded vessel A and the vessels were moored together for the cargo transfer. The mooring arrangement consisted of various lines belonging to vessel A.
During the loading process, Vessel B’s crew realised that Vessel A needed to be moved forward to accommodate the crane grab. At this point there was approximately an eight-metre difference in freeboard between the two vessels. Vessel B’s third
officer contacted Vessel A’s master via VHF radio, requesting the vessel to be moved forward by two to three metres. Vessel A’s master instructed the crew to proceed with the warping operation using spring lines. The master decided not to wake the
off-watch crew to assist to allow them to rest. However, he acknowledged the tiredness of the Chief Officer (C/O).
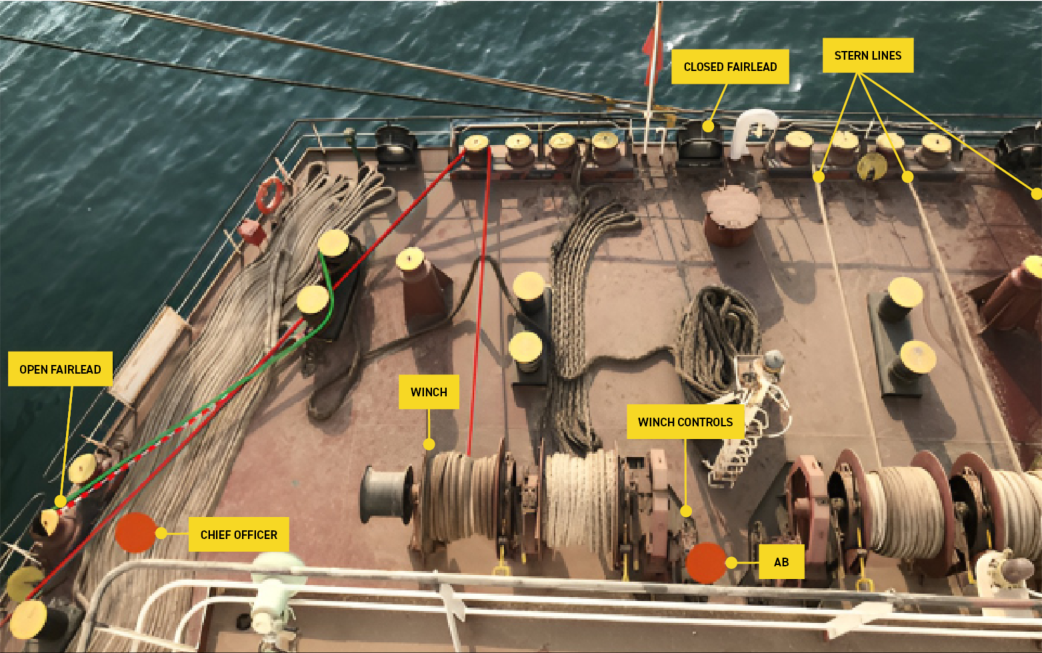
The warping operation began at 2234 with crew members positioned on the forward and aft mooring decks. The C/O and an able-bodied seafarer (AB) were on the aft mooring deck, preparing to heave the aft spring. As the forward springs were slackened, the AB started hauling the aft spring, intending to move Vessel A forward. However, as the mooring line came under tension, it unexpectedly sprang out of its shipside open roller fairlead, striking the C/O’s head and causing him to lose
consciousness.
The AB immediately notified the master via VHF radio about the C/O’s injury. The master instructed the crew to provide first aid and called for medical assistance from Vessel B, local VTS, the agent and the nearest Maritime Rescue Coordination Centre (MRCC). The C/O was unresponsive but was still breathing and a pulse was observed. The second officer administered first aid, including oxygen, and used a portable defibrillator.
The agent informed the master at 2255 that a local tug would evacuate the C/O ashore. The tug arrived at 2316 and the crew informed Vessel A’s master that they were awaiting permission from the local port authority before taking the C/O on board. The agent was also trying to organise the C/O’s evacuation by helicopter. The helicopter evacuation was ultimately not possible due to no helicopters being available and the C/O was transferred to the tug. The tug proceeded to port where a paramedic
assessed the C/O’s condition and confirmed he had passed away. A postmortem examination later revealed closed blunt force trauma to the head resulting in traumatic brain swelling and a brain haemorrhage as the cause of death.

Source MAIB REPORT 9/2022
Source MAIB REPORT 9/2022