
 English
EnglishThe BOSTON TRADER, a 9,528GT multipurpose dry cargo ship built in 2004 (Figure 1), was moored in the port of Oran, Algeria. While the crew were securing the containers loaded on deck, one seafarer was hit on the foot by the lower end of a falling lashing bar, which resulted in a serious injury and a toe being amputated.

Source: Investigation Report 04/2020 by Transport Malta
WHAT HAPPENED?
The BOSTON TRADER had been moored alongside the pier since 11 March 2019 and cargo operations were in progress. During the morning of 14 March 2019 the third officer (3/O), bosun (BSN) and two able bodied seamen (A/Bs) had been on watch since 0600. The bosun was keeping a watch on the ship’s gangway, while one AB (AB1) was securing the containers loaded on deck and another (AB2) was on the pier checking and sealing containers about to be loaded.
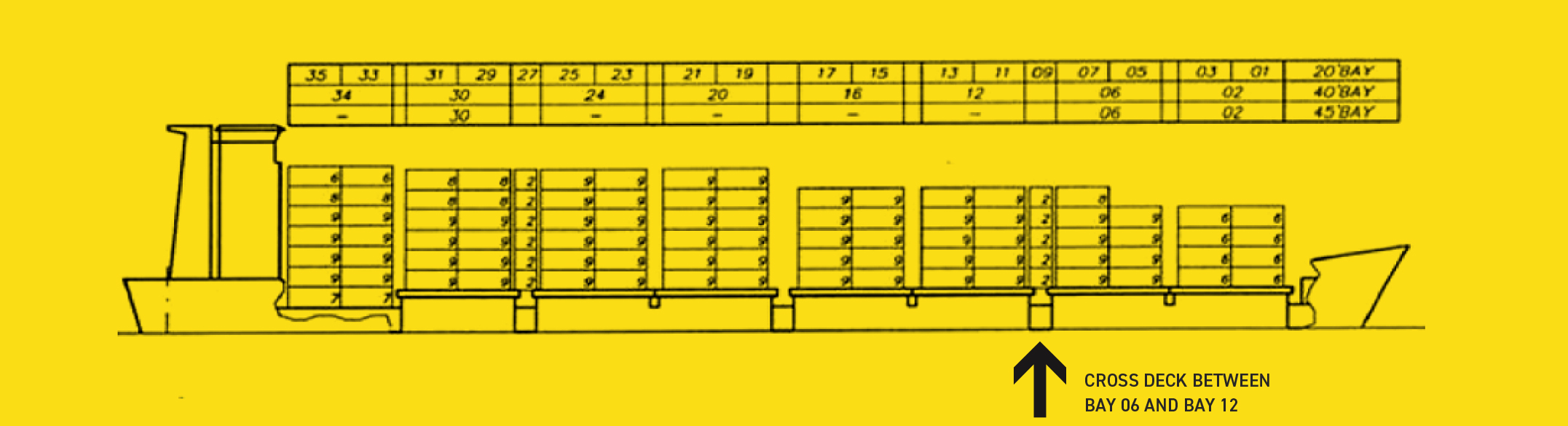
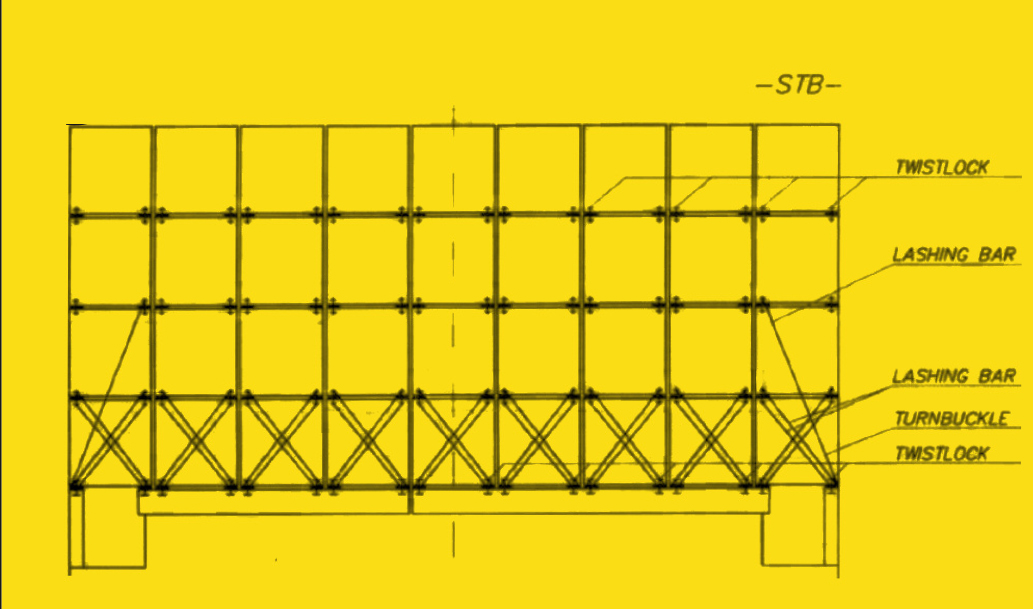
The containers loaded on deck were secured in accordance with the Cargo Securing Manual, which required the containers stowed on the hatch cover of No. 2 cargo hold (Bay 06), in the vicinity of where the accident occurred (Figure 2), to be secured as shown in Figure 3.
Source: Investigation Report 04/2020 by Transport Malta
Source: Investigation Report 04/2020 by Transport Malta
While the containers were being loaded, AB1 was positioned on the cross-deck between Bay 06 and Bay 12. The containers loaded on the third tier of the outboard ends had to be secured using a long lashing bar and tightened with a turnbuckle connected to it. The height of the long lashing bar was 5.07m and it was said to weigh more than 20kg.
The person securing the containers would usually have to step onto the hatch cover, using it as a pedestal, to hook the lashing bar into the corner fitting of a container (Figure 4). Once hooked, the lashing bar would have to be brought diagonally across to be connected to the turnbuckle, which would then be screwed down to tighten the securing arrangement.

Source: Investigation Report 04/2020 by Transport Malta
A 40ft container was loaded in Bay 06 on the third tier, towards the outboard end of the starboard side of the ship. In order to secure it, AB1 stepped onto the hatch cover of cargo hold No. 2 and hooked up a long lashing bar into the corner fitting of the container. While holding the hooked-up lashing bar with one hand, he then stepped down from the hatch cover onto the cross deck in order to lift the turnbuckle with the other hand.
At this point the lashing bar slipped out from the container socket and fell vertically down onto his right foot. The bottom end of the lashing bar cut through the safety footwear and injured his foot.
The chief officer (C/O), along with the BSN, arrived at the location and carried AB1 into the accommodation. The master informed the local agent of the accident and requested for emergency medical assistance, while the crew tried to stop the bleeding.
The agent, along with the local port authorities and a medical team, arrived on board. The medical team immediately transferred AB1 to a hospital ashore where he underwent surgery with one toe being amputated. Two days after the surgery the injured AB was discharged from the hospital and repatriated.
Further details about the incident and the lessons learned are provided in the summary of the case study.
In addition, a presentation and reflective learning form have been prepared based on the incident as suggested training materials. These can be used by Members or their crew in any way they see fit to encourage reflection and gain the maximum learning from this incident: to consider why the incident happened; “what it means to me”, and to then relate the identified learning points to one’s own personal situation.
Finally, a Britannia commentary on the incident has been prepared which discusses the key points in more detail in order to help develop the reflective learning from the case study.
CASE STUDY MATERIAL
BSAFE INCIDENT CASE STUDY NO.11 – SUMMARY
BSAFE INCIDENT CASE STUDY NO.11 – REFLECTIVE LEARNING FORM
LESSONS LEARNED
The following lessons learned have been identified. These are based on the information available in the investigation report and are not intended to apportion blame on the individuals or company involved:
- Risk control measures. The risk assessment available for the securing of containers required certain risk control measures to be put in place in order to minimise the associated risks. The investigation was of the view that some of these measures were not actually in place at the time of the incident.
- Correct application of PPE. The injured seafarer may have either worn his safety footwear improperly, or his foot slipped out at the time of the incident. Although he was wearing the right PPE and the correct size, the effectiveness of the safety shoes could have been compromised.
- Sufficient personnel for the securing of containers. Although the crew members believed that the securing of loaded containers could be carried out by only one person, taking into account the design of the lashing bar and the securing arrangements, the investigation found that at least two persons were required to secure the containers: one to hold the hooked up lashing bar and the other to connect it to the turnbuckle lying flat on the hatch cover.
- Slipping of the lashing bar from the corner fitting. The sockets of corner fittings into which lashing bars are hooked are oval in shape. A lashing bar, such as the one being used by the injured seafarer, was designed to slip easily into the socket of the container and to lock into the socket, once the bar is rotated diagonally across and connected to the turnbuckle. In view of this design, if the lashing bar is left suspended vertically, it may slip out from the socket of the corner fitting, especially if the lashing bar is not hooked correctly.
- Familiarisation with lashing arrangements and procedures. There were no records of any of the crew members being familiarised with the container securing procedures and arrangements of the ship. However, the injured seafarer had joined the ship three months prior to the incident and the ship regularly called at the port of Oran, where the securing of containers was always carried out by the crew members.
For more information on this incident email lossprevention@tindallriley.com.
THIS CASE STUDY IS DRAWN FROM THE INVESTIGATION REPORT PUBLISHED BY THE TRANSPORT MALTA MARINE SAFETY INVESTIGATION UNIT.
THE PURPOSE OF THIS CASE STUDY IS TO SUPPORT AND ENCOURAGE REFLECTIVE LEARNING. THE DETAILS OF THE CASE STUDY MAY BE BASED ON, BUT NOT NECESSARILY IDENTICAL TO, FACTS RELATING TO AN ACTUAL INCIDENT. ANY LESSONS LEARNED OR COMMENTS ARE NOT INTENDED TO APPORTION BLAME ON THE INDIVIDUALS OR COMPANY INVOLVED. ANY SUGGESTED PRACTICES MAY NOT NECESSARILY BE THE ONLY WAY OF ADDRESSING THE LESSONS LEARNED, AND SHOULD ALWAYS BE SUBJECT TO THE REQUIREMENTS OF ANY APPLICABLE INTERNATIONAL OR NATIONAL REGULATIONS, AS WELL AS A COMPANY’S OWN PROCEDURES AND POLICIES.