
 English
EnglishWhile at anchorage an electrician did not appear for dinner and consequently a search was initiated. He was later found trapped inside the vessel’s elevator shaft between the elevator’s counterweight and a protective beam, where he had been working earlier that same day. His fellow crew members managed to get him out of the elevator shaft, but, despite administering first aid, the electrician was pronounced dead at the scene.

Source: Investigation report 06/2018 by Transport Malta – Marine Safety Investigation Unit

Source: Investigation report 06/2018 by Transport Malta – Marine Safety Investigation Unit
WHAT HAPPENED?
During the voyage a potential problem was identified with the stopping position of the vessel’s elevator car. It was thought that the problem may be related to the elevator’s control cabinet overheating and possibly also to the adjustment of the elevator’s limit switches. Checks were carried out, but the problem persisted, and as a result the elevator was taken out of service until further investigation could be carried out at the next anchorage. On the morning of the incident a tool box meeting was conducted prior to starting the work. The meeting record indicated that the electrician and electro–technical trainee (ETT) would inspect the elevator’s speed governor and limit switches.
Signs were posted on each deck, and on the control panel, stating that the equipment was out of service due to maintenance. Similar signs were posted at the elevator’s call buttons on each deck and a public announcement was made to make the crew aware of the ongoing work on the elevator. As the work involved working in the elevator shaft, a ‘working aloft’ permit was issued.
The electrician and the ETT started checking and adjusting the limit switches working from deck E downwards. The electrician was working inside the elevator shaft, while the ETT was located outside to act as a safety/communications contact point. At 1645 local time the electrician and ETT stopped working to go for dinner. The elevator car was parked on Deck B and the ETT watched the electrician come down through the escape hatch in the roof of the car and exit through the open elevator door on Deck B. The electrician informed the bridge that both the ETT and himself were out of the elevator shaft and would continue the work the following morning.
On his way to the changing room on the upper deck, the EET noticed that the electrician had not followed him. At the time this did not raise any concerns as the EET assumed that the electrician had gone to his cabin to change for dinner. At about 1745 local time the electrician had still not arrived for dinner and the ETT expressed his concerns to the C/E. They both went to look for the electrician, but when they were unable to locate him, the C/E asked the ETT to point out where he had last worked with the electrician. They proceeded to the elevator door on B deck, which was closed. Upon opening the door using an emergency tool (Figure 1), they found that the elevator car had moved downwards. They could see the electrician inside the elevator shaft with his right leg draped over the counterweight and his upper torso trapped between the counterweight and one of the counterweight guard beams (Figure 2). It was noticed that the electrician was wearing a safety harness and he was outside the safety cage on top of the elevator car (Figure 3).

Source: Investigation report 06/2018 by Transport Malta – Marine Safety Investigation Unit
The C/E notified the master immediately, who raised the general alarm and then went to the bridge to inform the company. He also radioed the local authorities for medical assistance. A member of the onboard medical emergency team entered the elevator shaft and confirmed that the electrician was not breathing and he could not detect a pulse. Hoisting arrangements, using wires and chain blocks, were rigged, which allowed the elevator car to be hoisted and the counterweight to move down and free the electrician. At 1815 local time the electrician was pulled out from the elevator shaft and the 2nd Officer, who was the ship’s medical officer, confirmed that the electrician had no pulse.
The body was later taken ashore by boat and a post mortem confirmed the cause of death to be a blunt compressive trauma to the trunk. The company arranged for an authorised expert to carry out an inspection of the elevator. The inspection did not indicate any failure of the elevator’s machinery in relation to this particular incident.
Source: Investigation report 06/2018 by Transport Malta – Marine Safety Investigation Unit
Further details about the incident and the lessons learned are provided in the summary of the case study.
In addition, a presentation and reflective learning form have been prepared based on the incident as suggested training materials. These can be used by Members or their crew in any way they see fit to encourage reflection and gain the maximum learning from this incident: to consider why the incident happened; “what it means to me”, and to then relate the identified learning points to one’s own personal situation.
Finally, a Britannia commentary on the incident has been prepared which discusses the key points in more detail in order to help develop the reflective learning from the case study.
CASE STUDY MATERIAL
BSAFE INCIDENT CASE STUDY NO.12 – SUMMARY
BSAFE INCIDENT CASE STUDY NO.12 – REFLECTIVE LEARNING FORM
BSAFE INCIDENT CASE STUDY NO.12 – PRESENTATION
BSAFE INCIDENT CASE STUDY NO.12 – BRITANNIA COMMENTARY
LESSONS LEARNED
The following lessons learned have been identified. These are based on the information available in the investigation report and are not intended to apportion blame on the individuals or company involved:
- A safety cage is provided on top of the elevator car to safeguard the person(s). The electrician was found outside the safety cage, which may have exposed himself to additional danger.
- Earlier the electrician had left the elevator shaft through the emergency escape hatch of the car into the elevator cabin. This would have triggered the latch-out system and isolated the power on the system. To reactivate the elevator you would have to close the emergency escape hatch, and then physically reset the system at the control cabinet on deck D.
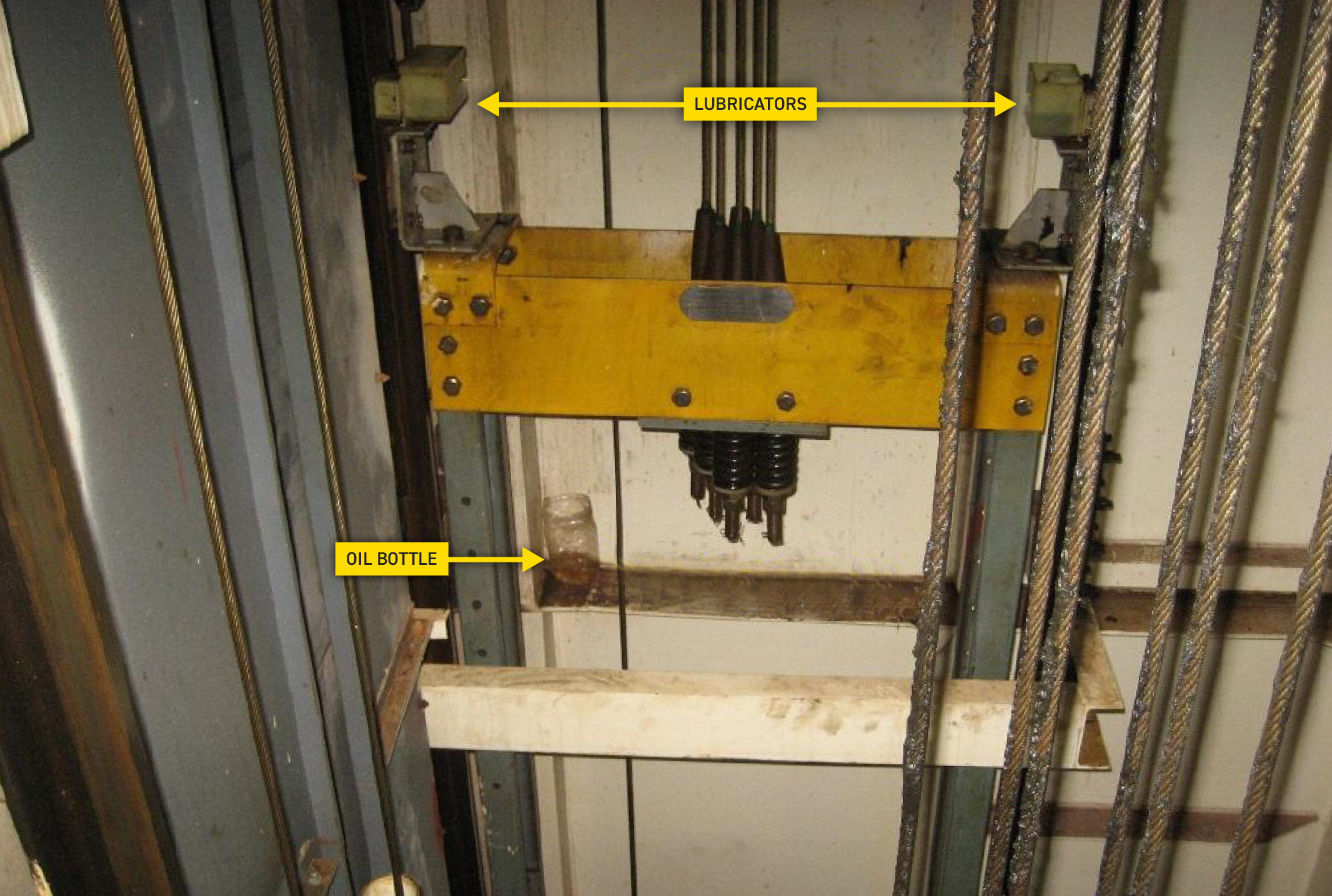
- From the position in which the electrician was found, the investigation hypothesised that he likely re-entered the elevator shaft to retrieve a plastic bottle containing oil used to top up the guide rail lubrication boxes (Figure 4). While trying to retrieve the bottle, it appears that he got trapped between the counterweight and the counterweight guard beam.
- The maintenance switch located at the safety cage was found in the “ON” position, meaning that the elevator could only be operated from there. The electrician was wearing a safety harness, which due to its attachment would have made him unable to reach the operation panel, indicating that the elevator was not intentionally operated from inside the shaft at the time of the incident.
- The manufacturer’s instructions state that if the elevator is not levelling at any floor, then it should be taken out of service and a technician consulted.
- While the onboard Safety Management system provided a risk assessment for ‘Electrical Workshop Activities on Elevator Cage’, this only covered the use of Personal Protective Equipment.
For more information on this incident email lossprevention@tindallriley.com.
THIS CASE STUDY IS DRAWN FROM THE INVESTIGATION REPORT PUBLISHED BY THE TRANSPORT MALTA MARINE SAFETY INVESTIGATION UNIT.
THE PURPOSE OF THIS CASE STUDY IS TO SUPPORT AND ENCOURAGE REFLECTIVE LEARNING. THE DETAILS OF THE CASE STUDY MAY BE BASED ON, BUT NOT NECESSARILY IDENTICAL TO, FACTS RELATING TO AN ACTUAL INCIDENT. ANY LESSONS LEARNED OR COMMENTS ARE NOT INTENDED TO APPORTION BLAME ON THE INDIVIDUALS OR COMPANY INVOLVED. ANY SUGGESTED PRACTICES MAY NOT NECESSARILY BE THE ONLY WAY OF ADDRESSING THE LESSONS LEARNED, AND SHOULD ALWAYS BE SUBJECT TO THE REQUIREMENTS OF ANY APPLICABLE INTERNATIONAL OR NATIONAL REGULATIONS, AS WELL AS A COMPANY’S OWN PROCEDURES AND POLICIES.