
 English
EnglishAn oil tanker was on passage when the ship’s electrician, who had been working alone, was fatally electrocuted while performing maintenance of the inert gas scrubber electrical system (Figure 1).
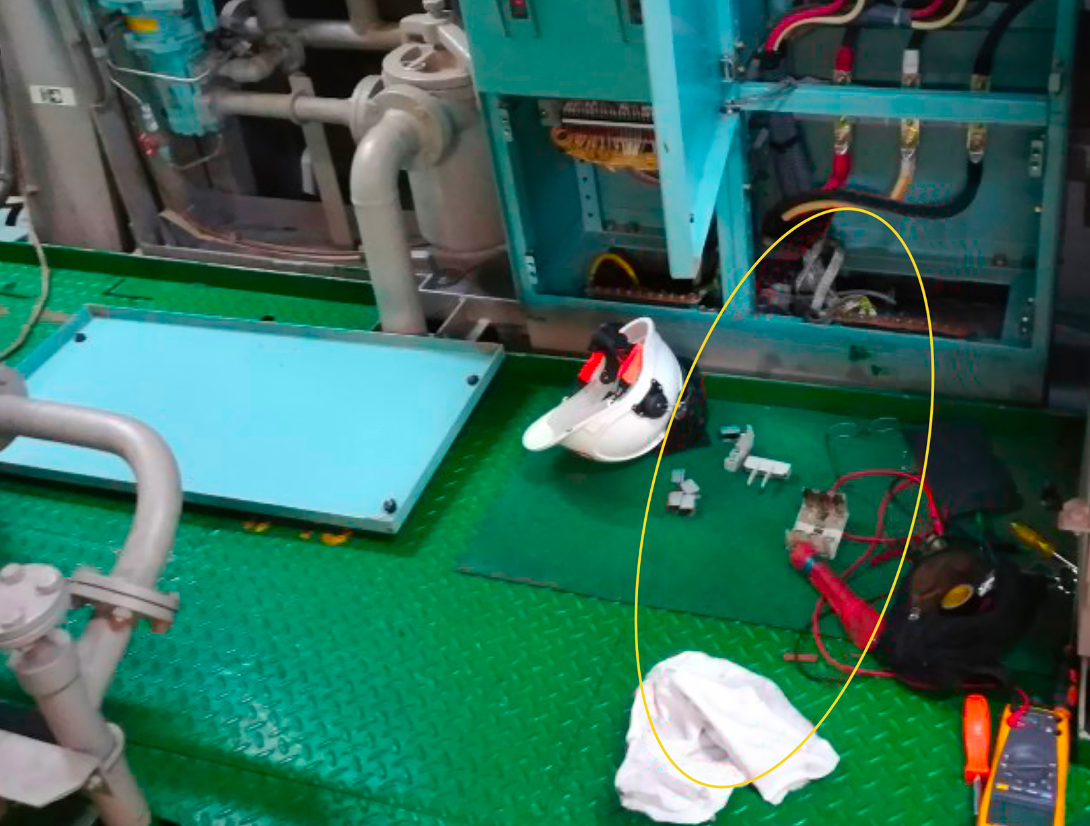
Figure 1 Location of the electrician when found.
Source: Investigation report by Republic of the Marshall Islands Maritime Administrator
WHAT HAPPENED?
Before starting work in the morning on the day of the incident, the second engineer (2/E) held a Toolbox Talk to discuss the work planned for that day. The electrician mentioned he might work on the inert gas (IG) scrubber pump starter panel, but he did not specify the items to be completed, nor the timeframe for the work. No formal risk assessment, permit to work (PTW) or Lock Out/Tag Out (LOTO) procedure were completed, despite all being specifically required by the Safety Management System (SMS).
At about 1130, the electrician told the engine cadet that he would be working on the IG scrubber pump starter panel. The cadet did not question the electrician about the work, nor did he tell any other engineering officer.
The IG scrubber pump starter panel was located on the engine room’s bottom platform inside a local group starter panel (LGSP) cabinet which had several sections: the upper sections held starter controls for various types of machinery, while the lower section contained the 440V power terminals. The cover over the power terminals was fully removable (Figure 2). The LGSP cabinet had no horizontal divider between the upper and lower section. Also the three power cable terminals in the lower section did not have covers over the power terminals to prevent accidental contact. The pump starter panel door could only be opened after turning the main power breaker lever to the off position, which de-energized the equipment in the panel.
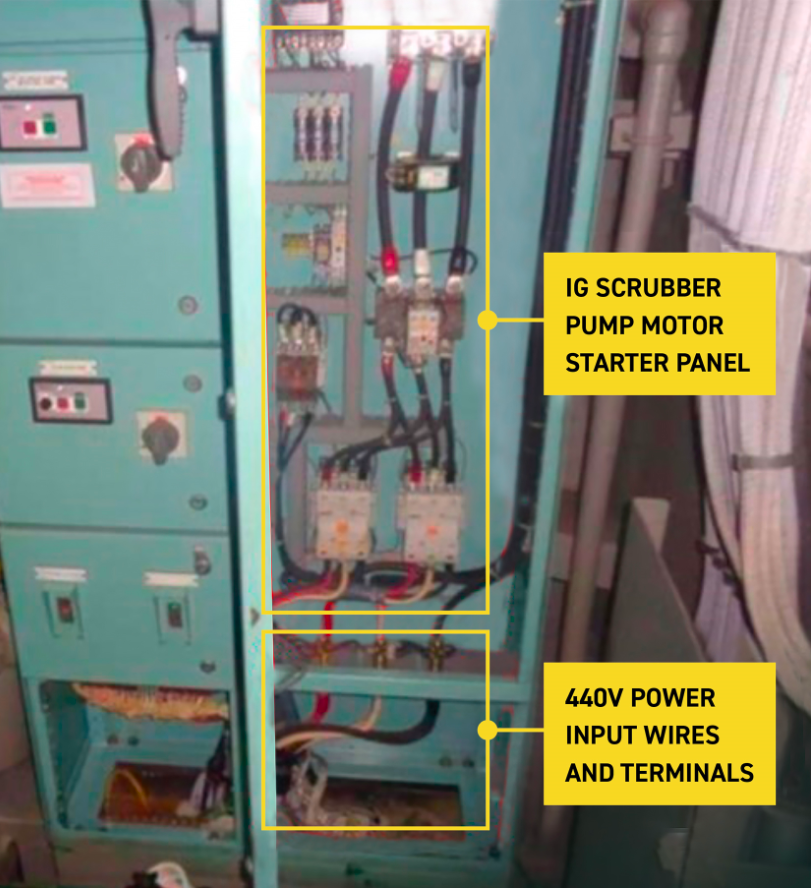
Figure 2 LGSP cabinet with IG scrubber pump starter panel open and power input terminal cover removed.
Source: Investigation report by Republic of the Marshall Islands Maritime Administrator
At 1144, the a low 440V insulation alarm activated in the engine control room (ECR), but the engine team could not identify the cause of the alarm. The cadet was instructed to tell the electrician to investigate the cause of the alarm and proceeded to the bottom platform where he had last seen him.
On arriving at the LGSP cabinet, the cadet found the unconscious and unresponsive electrician lying on the deck with his head and hands inside the lower section. The cadet removed the electrician from the LGSP cabinet by pulling on his safety shoes. The door for the IG scrubber pump starter panel was fully open, and the lower panel covering the 440V power terminals had been removed and placed to the left of the cabinet (Figure 1).
The cadet alerted the third engineer (3/E) and motorman working nearby. They then moved the electrician further away from the open LGSP cabinet, found he had no pulse and started cardiopulmonary resuscitation (CPR).
The master was subsequently advised, a general alarm raised and emergency medical equipment brought to the scene. Despite continued CPR, the electrician could not be resuscitated. The ship diverted to a nearby port, where the electrician was transported ashore the same day and pronounced dead. The cause of death was consistent with electrocution.
The main circuit breaker supplying power to the pump starter (inside the IG scrubber pump starter panel) was found in the off (open) position. The star contactor for the pump starter was missing a spring and cover locking pin (Figure 3). These were found on the cabinet’s lower framing and deck. The investigation presumed that the electrician inadvertently touched the energized 440V power terminals in the cabinet’s lower section while retrieving the star contactor spring or the cover locking pin.

Figure 3 IG scrubber pump starter contacts and the missing star contactor spring.
Source: Investigation report by Republic of the Marshall Islands Maritime Administrator
Further details about the incident and the lessons learned are provided in the summary of the case study.
In addition, a presentation and reflective learning form have been prepared based on the incident as suggested training materials. These can be used by Members or their crew in any way they see fit to encourage reflection and gain the maximum learning from this incident: to consider why the incident happened; “what it means to me”, and to then relate the identified learning points to one’s own personal situation.
Finally, a Britannia commentary on the incident has been prepared which discusses the key points in more detail in order to help develop the reflective learning from the case study.
CASE STUDY MATERIAL
BSAFE INCIDENT CASE STUDY NO.4 – SUMMARY
BSAFE INCIDENT CASE STUDY NO.4 – REFLECTIVE LEARNING FORM
LESSONS LEARNED
The following lessons learned have been identified based on the information available in the investigation report and are not intended to apportion blame on the individuals or company involved:
- A formal risk assessment, as required by the SMS, should have identified the hazards of working in the cabinet with 440V power cables and terminals, and would have resulted in adequate risk mitigation.
- Completing a PTW, as required by the SMS, would have resulted in the LOTO procedures being applied, ensured that the circuits and equipment in the work area were de-energized. They would have also prevented the electrician from accessing the cabinet while the 440V power input was not secured.
- A work-specific Toolbox Talk could have helped with appropriate pre-task hazard identification. The engineering officers were reportedly unaware that the electrician was completing this work and a Toolbox Talk had not been held with him.
- The Company’s SMS required that all scheduled work be planned at least one day in advance to allow time for completing the required safety procedures. During the morning planning meeting, the electrician was not questioned or prevented from undertaking the unplanned work.
- The electrician was working alone when the incident occurred. A completed PTW would have required another crew member to be present, which could have resulted in an appropriate challenge and stopped the unsafe work.
- The Company’s Stop Work Authority (SWA) policy required all crew members to take action to prevent observed unsafe acts or conditions. Using this authority, the 2/E and engine cadet could have prevented the electrician from undertaking the task.
- An effective and timely scheduled maintenance would have resulted in recording and rectifying the missing physical safety barriers within the LGSP cabinet and prevented the electrician from accidental contact with energized circuits.
- Although it did not contribute to the incident, the cadet could also have been electrocuted when he immediately pulled the electrician from the LGSP cabinet, as he had not ensured that the power was isolated or that the electrician’s body was not energized.
The source of this case study is an investigation conducted by the Republic of the Marshall Islands Maritime Administrator.
The purpose of this case study is to support and encourage reflective learning. The details of the case study may be based on, but not necessarily identical to, facts relating to an actual incident. Any lessons learned or comments are not intended to apportion blame on the individuals or company involved. Any suggested practices may not necessarily be the only way of addressing the lessons learned, and should always be subject to the requirements of any applicable international or national regulations, as well as a company’s own procedures and policies.