
 English
EnglishWhile on passage at night, a 2,281gt general cargo ship ran aground on the Pentland Skerries in the eastern entrance of the Pentland Firth, Scotland (Figure 1). The ship sustained significant hull damage, but there was no pollution or injuries.

WHAT HAPPENED?
On the afternoon before the grounding, while on passage, a bridge team meeting was held to discuss the forthcoming transit of the Pentland Firth, a stretch of water to the north of the Scottish mainland notorious for extreme tidal and sea conditions. The master decided to adjust the bridge watchkeeping schedule in order to make the transit in favourable tidal conditions. The cadet was directed to keep watch from 2300 to 0200 (all times UTC + 2) and the maritime officer would then commence his watch with the transit of the Pentland Firth due to begin at about 0500.
Between about 1730 and 1900 the maritime officer had dinner and consumed two beers in the mess room. He went to his cabin at about 1900 and slept from approximately 2130 until 0145.
The maritime officer relieved the cadet as officer of the watch (OOW) at 0200 with the ship making 7.8kts on a heading of 280° in calm seas. The ship had been on track mode steering, which enables it to automatically follow its planned track. However, the maritime officer deselected this and switched to the standalone autopilot and set the heading to 279°.
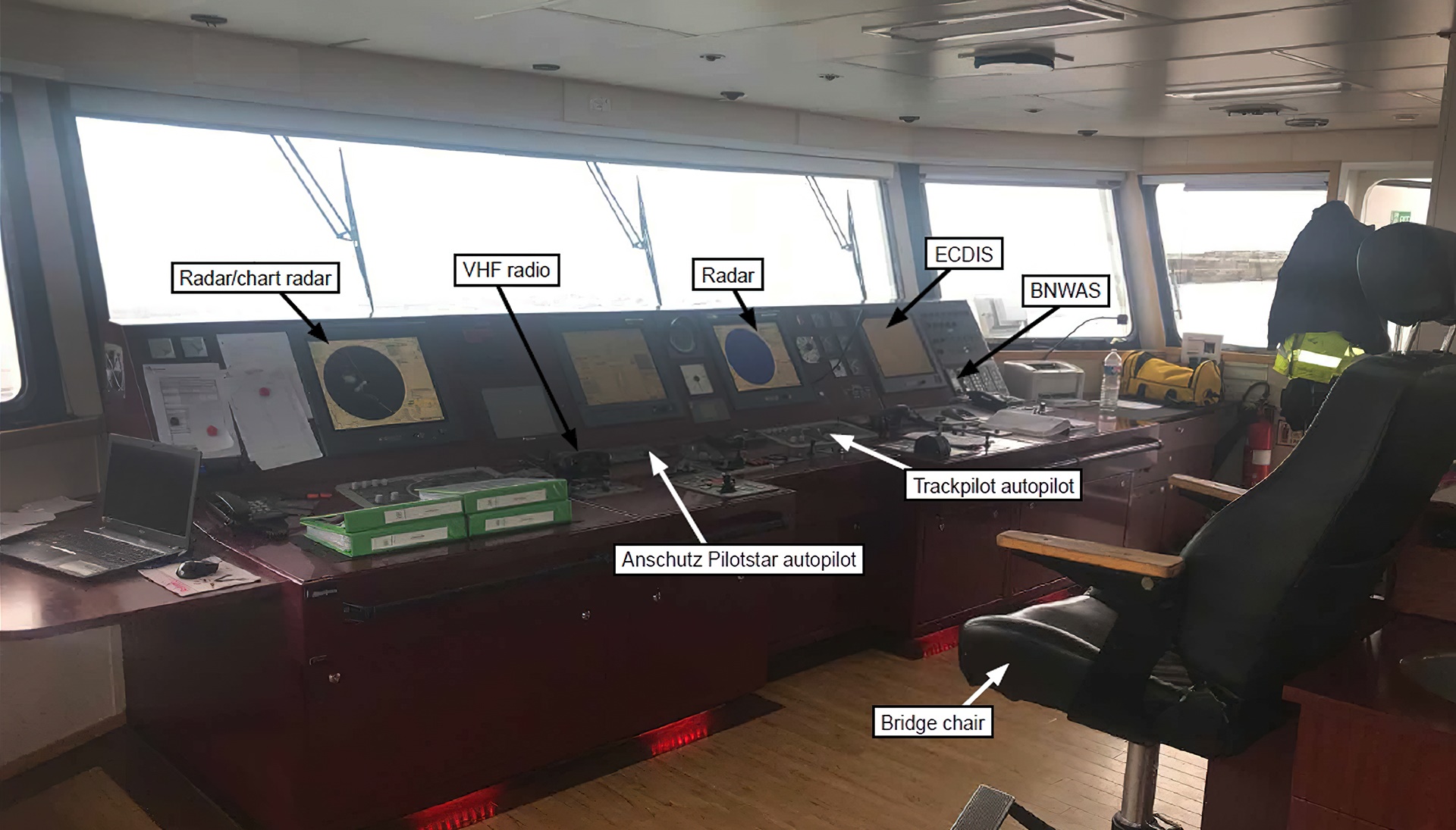
ALONE ON THE BRIDGE, HE THEN SAT DOWN IN THE BRIDGE CHAIR (FIGURE 2) AND STARTED WATCHING MUSIC VIDEOS ON HIS MOBILE PHONE. THE BRIDGE NAVIGATION WATCH ALARM SYSTEM (BNWAS) WAS NOT IN USE.
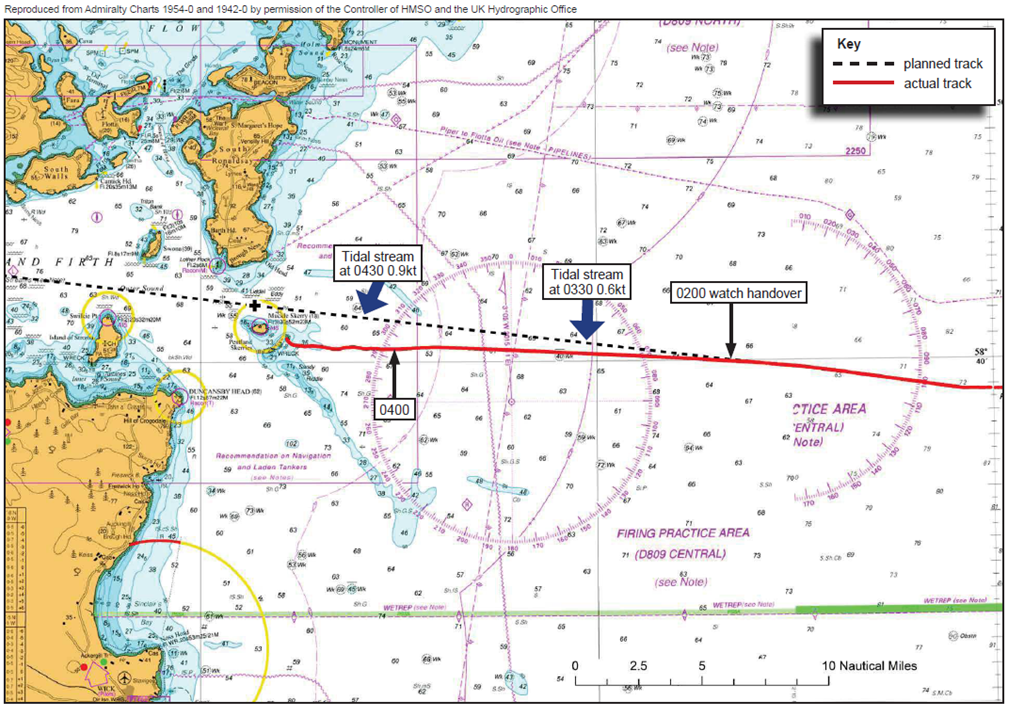
At about 0400 the OOW looked at the radar and realised that the ship was south of the planned track (Figure 3). At the same time he observed two small islands ahead on the radar. He decided to proceed between the islands and after which he intended to alter course to starboard to regain the planned track.
At 0427 an Orkney Vessel Traffic Service Officer (VTSO) observed the vessel on his radar heading towards the shallow waters of the Pentland Skerries and contacted the Shetland Coastguard Operations Centre (CGOC). The CGOC watch officer then contacted the ship by VHF and queried whether the OOW was aware of the islands two miles ahead. The OOW acknowledged the situation and confirmed that the ship was “two miles from the course change”. When the CGOC watch officer sought further confirmation that the OOW intended to alter course to avoid the rocks, the OOW replied that “we will see later”.
The VTSO continued to monitor the ship but did not observe any alteration of course. At 0440 he therefore contacted the ship directly by VHF and emphasised that a grounding on the rocks five cables ahead was imminent and that there was clear water to the south. The OOW acknowledged the impending danger and indicated that he would change course, but his response was confused.
During the conversation, the OOW reduced the range scale on his radar and added a chart overlay to the display.
AT THIS POINT HE REALISED THAT THE PROPOSED COURSE BETWEEN THE TWO ISLANDS AHEAD WAS UNSAFE AS THERE WAS A SHALLOW REEF BETWEEN THEM. HE THEREFORE SELECTED HAND-STEERING AND PUT THE RUDDER HARD TO STARBOARD TO TRY TO STEER AWAY FROM THE REEF.
However, at 0443 the ship grounded on the Pentland Skerries at a speed of 7kts (Figure 4). The sea was calm with light airs and good visibility in darkness. The ship sustained extensive damage to its hull and was refloated seven days later.

Further details about the incident and the lessons learned are provided in the summary of the case study.
In addition, a presentation and reflective learning form have been prepared based on the incident as suggested training materials. These can be used by Members or their crew in any way they see fit to encourage reflection and gain the maximum learning from this incident: to consider why the incident happened; “what it means to me”, and to then relate the identified learning points to one’s own personal situation.
Finally, a Britannia commentary on the incident has been prepared which discusses the key points in more detail in order to help develop the reflective learning from the case study.
CASE STUDY MATERIAL
BSAFE INCIDENT CASE STUDY NO.3 – SUMMARY
BSAFE INCIDENT CASE STUDY NO.3 – REFLECTIVE LEARNING FORM
LESSONS LEARNED
The following lessons learned have been identified based on the information available in the investigation report and are not intended to apportion blame on the individuals or company involved:
- The ship grounded because it drifted to the south of the planned track while on autopilot. The OOW did not monitor the ship’s progress for about two hours, while sitting in the bridge chair watching videos on his mobile phone.
- The ECDIS was not fully utilised and a number of navigational alarms could have been used to warn the OOW of the danger. If the bridge navigational watch alarm system had been switched on, this would have assisted the OOW to keep alert.
- The posting of an additional lookout would have further assisted the OOW by providing navigational support as well as potentially helping the OOW to remain alert.
- An effective risk assessment taking into account the proximity of navigational hazards while operating at night would have identified the need to retain an additional lookout.
- Although there should have been sufficient time to regain the planned route when the OOW realised that the ship was off track, he did not refer to all navigational information and instead chose a route between the islands that placed the ship in imminent danger.
- The ship’s OOW responded to two verbal warnings of the danger from shore authorities, but the resulting action he took was not effective, indicating that his situational awareness had been affected, nor did he call the master to assist.
- The inclusion of meaningful details describing the navigational hazards in the passage plan would have increased the OOW’s awareness of the risks and helped him monitor progress.
- The ship’s Safety Management System (SMS) was deemed to provide insufficient guidance to support the safe conduct of navigation and did not have a policy regarding the use of personal electronic devices during watchkeeping.
This case study is drawn from the investigation report 12/2019 published by the Marine Accident Investigation Branch.
The purpose of this case study is to support and encourage reflective learning. The details of the case study may be based on, but not necessarily identical to, facts relating to an actual incident. Any lessons learned or comments are not intended to apportion blame on the individuals or company involved. Any suggested practices may not necessarily be the only way of addressing the lessons learned, and should always be subject to the requirements of any applicable international or national regulations, as well as a company’s own procedures and policies.