
 English
EnglishA FULLY CELLULAR 1,400 TEU / 25,000 GT CONTAINER SHIP WAS ON A VOYAGE FROM MELBOURNE TO FREEMANTLE, AUSTRALIA, WHEN WATER WAS FOUND IN AN UNDERDECK PASSAGE. IT TRANSPIRED THAT DURING HEAVY WEATHER THE HATCH ACCESS LID ON THE FORECASTLE DECK LEADING TO THE FORECASTLE STORE HAD BEEN RIPPED OFF AND DUMPED ON THE WINDLASS, ALLOWING WATER INGRESS INTO THE FORECASTLE. WHILE ATTEMPTING TO RIG A TEMPORARY ARRANGEMENT TO STOP FURTHER WATER INGRESS, A LARGE WAVE CRASHED ONTO THE FORECASTLE DECK, INJURING THREE CREW MEMBERS. THE CHIEF OFFICER WAS SEVERELY INJURED AND SUCCUMBED TO HIS INJURIES BEFORE MEDICAL ASSISTANCE FROM ASHORE COULD ARRIVE.
WHAT HAPPENED
While on passage across the Great Australian Bight from Melbourne to Freemantle, the ship encountered heavy weather. The weather had deteriorated during the previous night as a front passed over, necessitating a reduction in the main engine speed. At the time of the incident a Beaufort Force 7 (28 – 33 knots) wind was blowing with a very rough sea and a long, heavy swell. The vessel was riding the weather well and only occasionally shipping spray forwards.
At 0800 the captain, following a discussion with the chief officer and third officer, felt that the weather was getting slightly better and there was no need to restrict access to the main deck. However, the third officer had previously instructed the watchkeeping able bodied seafarer (AB), who was also working on stencilling the ship’s new name on the lifebuoys, not to do any work on the forecastle.
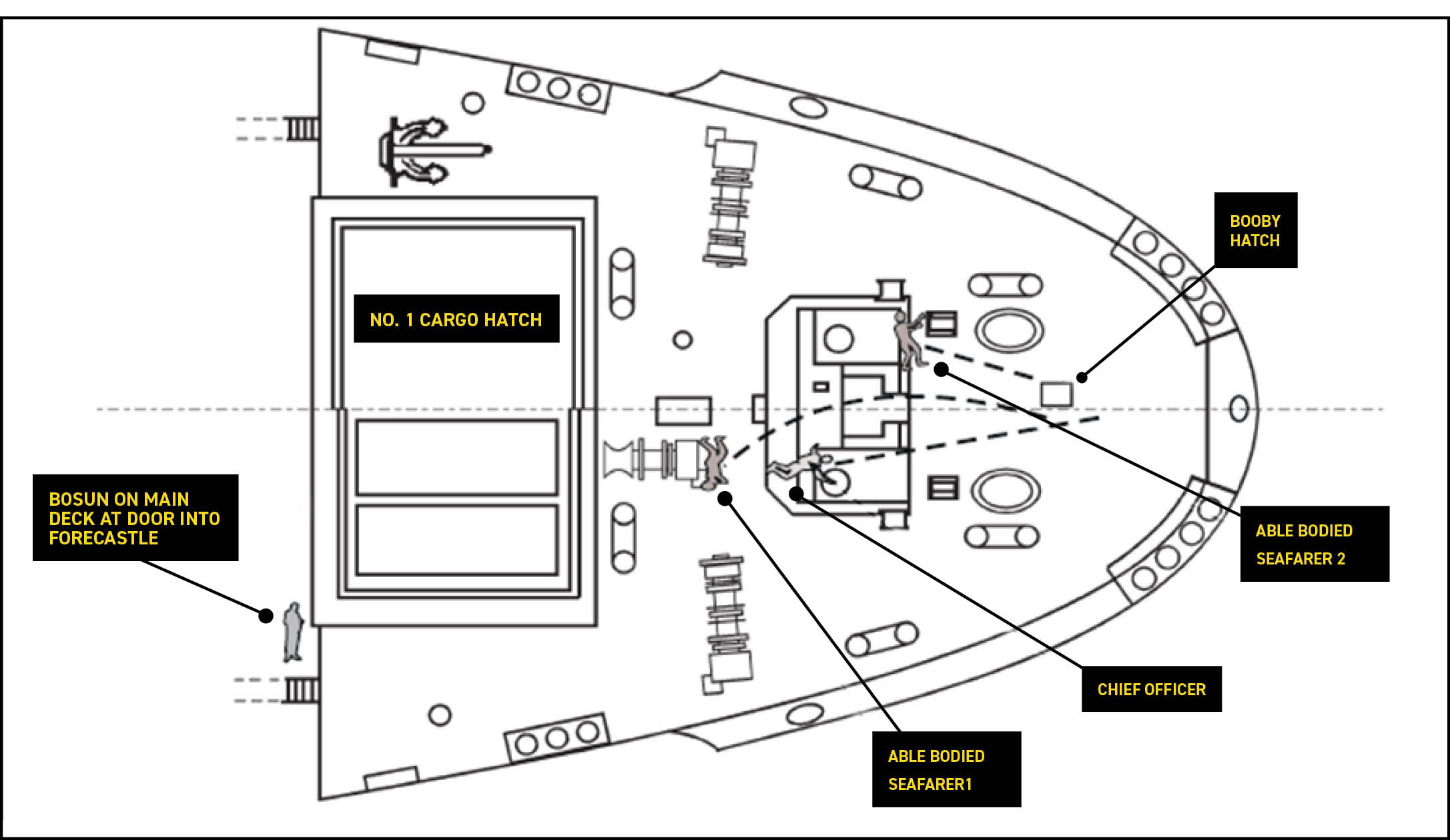
At 0800 the second engineer reported by telephone to the chief officer on the bridge that he could see sunlight in the forecastle store, coming through the access hatch on the forecastle deck. This had been discovered following the electrician, when proceeding to the cargo holds to check on the refrigerated containers, reporting the presence of water at the aft end of the port side underdeck passage to the second engineer who in turn investigated the source of the water. It is believed that the chief officer had, following his earlier conversation with the second engineer, initially proceeded by himself to the forecastle to investigate, prior to returning to the accommodation where he engaged the assistance of three crew members, the bosun and two ABs, to proceed forwards to assist him. Due to the containers on deck, the party proceeding along the deck and onto the forecastle were not visible to the bridge watchkeeper and the chief officer had not informed the bridge, or anyone else of his plan, and none of them had a radio. Others on the bridge did not know what the phone call between the second engineer and the chief officer was about. The party of four proceeded to the forecastle (FIGURE 1) via the main deck.

The repair party found that the access hatch cover to the forecastle store had been torn off and was lying on top of a gypsy. Ropes previously coiled abaft the windlass were found scattered around the deck. These were coiled and lashed before the issue of the damaged access hatch was addressed. The access hatch lid was found to be distorted and attempts to replace it proved fruitless. The chief officer then instructed the bosun to get some canvas with which they could make a temporary cover for the access. Due to the updraught emanating from the forecastle store through the access hatch coaming, securing the access with a canvas cover alone was found to be problematic. Therefore, the bosun was sent to get some plywood and he went back into the forecastle store. Meanwhile the two ABs refitted the spurling pipe covers which had also been washed off and then went to secure the damaged hatch lid under the windlass. Shortly afterwards, with the ABs standing either side of the damaged hatch lid ready to lift it, and the chief officer standing forward of them, facing aft (FIGURE 2), one of the ABs felt the bow notably lift and spotted a large wave approaching.

The AB shouted a warning and, although he held on tight to a forestay, the force of the wave which crashed onto the forecastle tore his grip from the forestay and washed him over the windlass and he crashed against a mooring winch behind. The other AB was washed against the windlass on the port side, suffering leg injuries, and the chief officer was washed under the windlass (FIGURE 3). Although stunned and having sustained a head injury, the AB who had been washed over the windlass called out to his colleagues and, upon receiving no reply, he believed they had been washed overboard.
He went to find the bosun, who subsequently sent him to notify the bridge that they had personnel overboard. The bridge then sounded the man overboard alarm and commenced a Williamson turn. While the search for the two apparently missing men commenced, the second AB on the forecastle recovered slightly and found the chief officer under the windlass (FIGURE 4). He made his way to advise the bosun of the chief officer’s location.
The chief officer was evacuated to the ship’s hospital by stretcher, where it was found he had a broken leg and severe chest and head injuries. He succumbed to his injuries later that day.

LESSONS LEARNED
The following lessons learned have been identified. These are based on the information available in the investigation report and are not intended to apportion blame on any individuals or the company involved.
- The chief officer had not told the captain and bridge watchkeeper of the damage, or of his intention to proceed to the forecastle to firstly investigate and secondly make temporary repairs.
- No one in the repair party took a radio with them to maintain contact with the bridge.
- Access to the main deck had not been restricted, as it was believed the weather had slightly improved. However, in reality, it still posed a notable risk to personnel on deck.
- No risk assessment had been carried out prior to the chief officer, and later the chief officer and three crew, proceeding to the forecastle.
- As the bridge team were unaware of the crew on the forecastle to conduct repair efforts, the vessel’s course and speed was not altered to reduce the risk of sea water on deck.
- There was confusion in relation to reports of crew overboard, as a crew member, in a time of a high stress and shock, reverted to his mother tongue and could not be understood by the bridge watchkeeper, which led to uncertainty as to whether personnel had been washed overboard.
- The telephone system was made inoperable when one handset was left “off the hook” and this had also happened two times the previous day with telephone handsets displaced due to the heavy weather. This hampered the bridge watchkeeper’s ability to contact the captain following the reports of a man overboard.
- The securing dogs on the access hatch had been fitted by the bosun upon departure from Melbourne. However, they had only been secured hand tight. The access hatch cover hinges were on the aft side of the hatch and therefore any lack of tightness would have made the hatch susceptible to damage with each successive wave crashing across the access hatch. The hatch cover had also been torn off around six months previously, so to try and stop this happening again a pad eye had been welded on to the underside of the hatch with the aim to connect to a rung of the ladder underneath with a bottle screw (FIGURE 5). On this occasion the additional securing device had not been fitted. When the hatch cover was repaired in port following the fatal incident, the hatch was rotated 180˚ and the hinge fitted on the forward side of the coaming/hatch.
- The reason that the water ingress was originally seen by the electrician was because the watertight door at the forward end of the port underdeck passage into the forecastle had been left open. These doors were apparently regularly being left open on the vessel, negating its watertight integrity if the forward part of the vessel were to be damaged. Furthermore, there were no warning signs on the doors advising that these should be kept closed at sea, except for access.
For more information on this incident email lossprevention@tindallriley.com
THIS CASE STUDY IS DRAWN FROM THE INVESTIGATION REPORT PUBLISHED BY THE MARINE INVESTIGATION UNIT – AUSTRALIA
THE PURPOSE OF THIS CASE STUDY IS TO SUPPORT AND ENCOURAGE REFLECTIVE LEARNING. THE DETAILS OF THE CASE STUDY MAY BE BASED ON, BUT NOT NECESSARILY IDENTICAL TO, FACTS RELATING TO AN ACTUAL INCIDENT. ANY LESSONS LEARNED OR COMMENTS ARE NOT INTENDED TO APPORTION BLAME ON THE INDIVIDUALS OR COMPANY INVOLVED. ANY SUGGESTED PRACTICES MAY NOT NECESSARILY BE THE ONLY WAY OF ADDRESSING THE LESSONS LEARNED, AND SHOULD ALWAYS BE SUBJECT TO THE REQUIREMENTS OF ANY APPLICABLE INTERNATIONAL OR NATIONAL REGULATIONS, AS WELL AS A COMPANY’S OWN PROCEDURES AND POLICIES.