
 English
EnglishA small ship (Figure 1) was chartered to carry a cargo of corn on a short haul voyage in Europe. On completion of loading, aluminium phosphide was placed in the holds to fumigate the cargo in transit. On the second day of the voyage, while the ship was experiencing heavy weather, hydrogen phosphide gas (PH3) entered the accommodation area via a hydraulic room. The fumigant was not detected in time to avert lethal levels of exposure. Several members of the crew were overcome with one crew member dying and three others having to be evacuated.

Source: Investigation report by The Bahamas Maritime Authority
WHAT HAPPENED?
The ship (Figure 1) was a 3,000 tonnes DWT general cargo vessel built in 1994 with a single box-shaped cargo hold equipped with movable bulkheads. The accommodation consisted of two decks, of which the lower was below the main deck level. The forward bulkhead of this deck was next to the cargo hold.
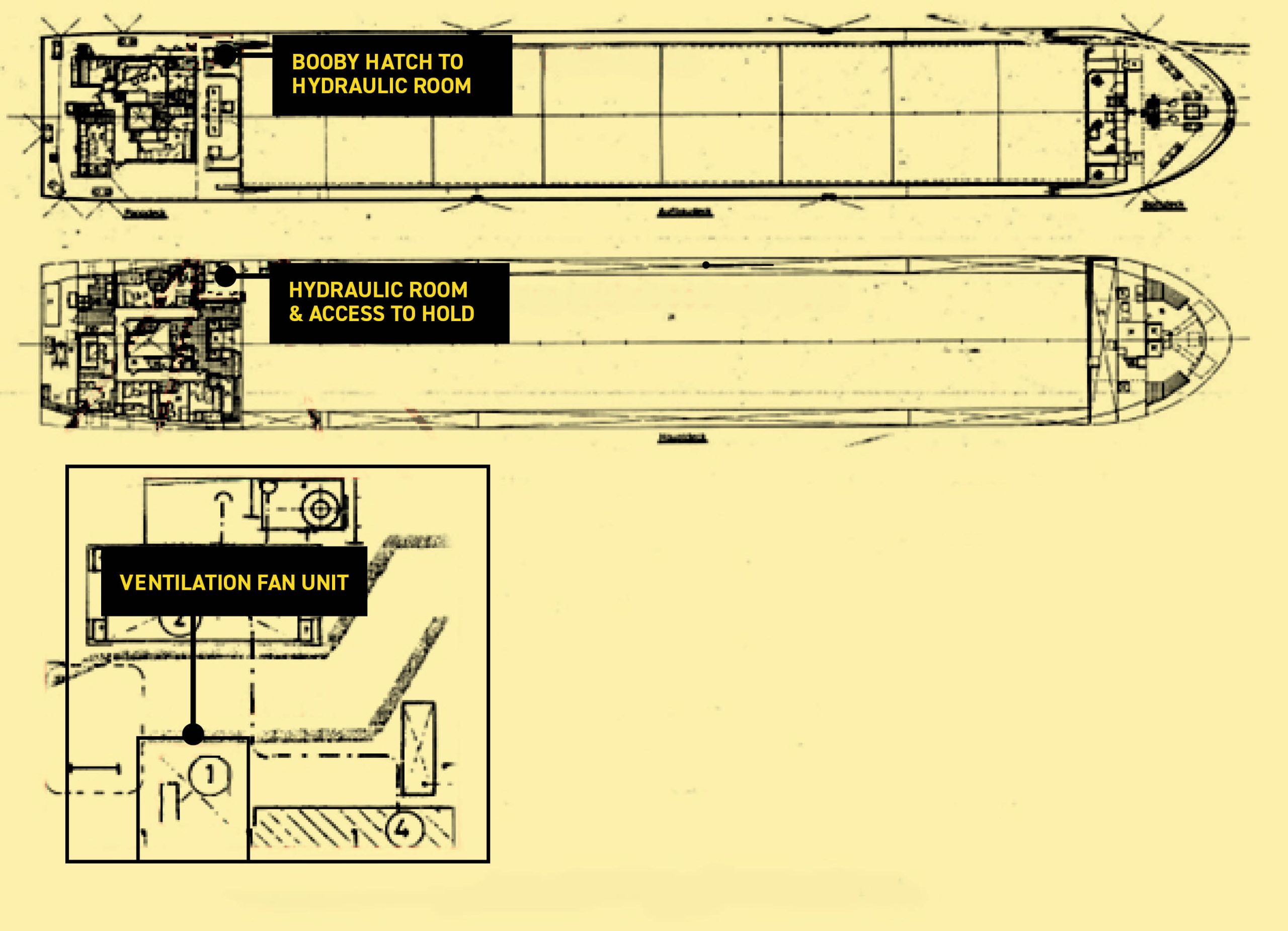
Access to the cargo hold was gained through a booby hatch at the front and through a hydraulic room aft (Figure 2). The hydraulic room shared two bulkheads with the accommodation space. The ventilation of the cargo hold was arranged via ducts forward and aft. The aft ventilation duct passed through the accommodation space and was adjacent to the engine room air intakes.
On 11 February 2020 the ship berthed in Sables d’Olonne, France, to load a cargo of 2,750 tonnes of corn in bulk. After preparation of the hold, the space was inspected by cargo interests to gauge the suitability for cargo and, after additional cleaning, loading commenced that afternoon. The hold’s gas tight integrity was not assessed by the charterers or the ship’s crew.
After the loading was completed at around 2145, technicians from a fumigation company visited the ship and made preparations for fumigation. After verbally confirming with the master that the hold was suitable for fumigation, three bags of aluminium phosphide were placed in the hold to provide the required dose of the fumigant. The hatches were then closed and the master was given a briefing document pack and equipment for testing for the presence of the fumigant inside the accommodation space and engine room. The chief officer (C/O) was given training in the use of the gas detection equipment provided.
Source: Investigation report by The Bahamas Maritime Authority
The compound used to fumigate the cargo was aluminium phosphide, which creates the fumigant, phosphine gas (PH3). For in-transit fumigation, the compound is placed on top of the cargo on completion of loading. As phosphine gas is heavier than air, the gas sinks penetrating the cargo during the voyage. The amount of compound required is calculated using the volume of the cargo and the size of the cargo hold. Phosphine gas is flammable, colourless and odourless. However, the addition of chemicals to the compound gives the gas the odour of garlic to provide a warning. In the case of exposure, there is no antidote; the treatment is to provide oxygen.
The ship remained alongside overnight waiting for the tide and departed for Hull in the UK at 0600 the next morning. An initial check for the presence of the fumigant was conducted by the C/O at 0800 at two locations in the accommodation space and one in the engine room. These checks were then repeated at 2000 and 0800 the following day (13 February).
Meanwhile the weather deteriorated and the master adjusted the passage plan accordingly. At approximately 1030 on 13 February, a wave entered the ventilation trunking which resulted in water flooding the galley and a store room. The ventilation system was then stopped and the accommodation’s ventilation flaps were shut. For a period in the early afternoon, the combination of the apparent wind direction and the openings on the bridge and accommodation resulted in exhaust gas being funnelled into the accommodation.
After lunch the crew who were not working retired to their cabins. By 1245 several of the crew were experiencing headaches, fatigue and severe nausea which they attributed to seasickness, reaction to the food served at lunch or the presence of exhaust gas in the accommodation. With the exception of the chief engineer (C/E), who went to the engine room, the crew affected either remained in their cabins, went to the bridge or went on to the boat deck to get fresh air.

It was not until around 1800 when the master became aware that at least three of the crew were unwell and the possibility of fumigation poisoning was raised. The information provided by the fumigation company was then re-checked and the master tested the atmosphere in the accommodation and confirmed the presence of the fumigant gas (PH3).
At 1833 the second officer (2/O) phoned local authorities to report the presence of the fumigant in the accommodation and requested assistance. The crew were then moved to the ship’s office and master’s cabin where windows could be opened to increase the flow of fresh air. Sometime before 1900, the able bodied seaman/cook (AB/Cook) returned to his cabin for an unknown reason, which was unnoticed.
At 2019 a rescue helicopter reached the ship and a winchman was lowered on to the deck. However, the helicopter had to return to base without the crew affected and the winchman due to the weather conditions combined with a technical issue. The ship then re-routed to Brest in France.
At 2059 the winchman reported to shore that three members of the crew were in a serious condition and that the AB/Cook had been found dead in his cabin.
About an hour later a second helicopter arrived with a medical team and stabilised the three crew, who were evacuated by boat when the ship arrived at Brest and eventually recovered in hospital.
After the incident an investigation using pressure checks and smoke testing revealed no leaks on the cargo hold’s aft bulkhead or in the ventilation duct. However, the following issues were identified in the hydraulic room:
- The door leading from the hydraulic room to the cargo hold was misaligned and could not be made gas-tight, even with all dogs adjusted.
- A ventilation fan and the associated trunking running through the hydraulic room was not airtight. This ventilation system extracted air from the accommodation’s sanitary spaces and vented on deck. With the fans stopped, a smoke generator located in the hydraulic room filled the accommodation space in under a minute.
- There were also two uncapped stubs of unused small diameter pipe running between the hydraulic room and the accommodation.
Further details about the incident and the lessons learned are provided in the summary of the case study.
In addition, a presentation and reflective learning form have been prepared based on the incident as suggested training materials. These can be used by Members or their crew in any way they see fit to encourage reflection and gain the maximum learning from this incident: to consider why the incident happened; “what it means to me”, and to then relate the identified learning points to one’s own personal situation.
Finally, a Britannia commentary on the incident has been prepared which discusses the key points in more detail in order to help develop the reflective learning from the case study.
CASE STUDY MATERIAL
BSAFE INCIDENT CASE STUDY NO.13 – SUMMARY
BSAFE INCIDENT CASE STUDY NO.13 – REFLECTIVE LEARNING FORM
LESSONS LEARNED
The following lessons learned have been identified. These are based on the information available in the investigation report and are not intended to apportion blame on the individuals or company involved:
- The company‘s Safety Management System (SMS) did not contain any guidance on the carriage of fumigated cargo and did not include any procedures to ensure the ship was suitable for in-transit fumigation prior to accepting the charter.
- No risk assessment for the carriage of fumigated cargoes was conducted and no contingency plans had been developed in the event of fumigant ingress in to the accommodation.
- Checks on the ship’s suitability and gas tight integrity were limited to verbal confirmation with the master and C/O that the hold did not have any known issues, a hold smoke-sampling system or any open connection with the engine room or duct keel. The SMS did not provide any guidance on maintaining gas tight integrity of the cargo hold, or conducting a pre-loading inspection.
- The fumigators did not arrive at the ship until after loading was complete and, as such, this inspection could not be conducted as required. No inspection was made by the ship’s staff to confirm the gas tight integrity of the hold.
- The hydraulic room/hold door was not gas or watertight. This had not been identified as part of the ship’s planned maintenance schedule.
- Only one crew member (the C/O) was provided with training by the fumigator-in-charge. In turn, the C/O’s briefing for the crew did not adequately highlight the risk of the operation or the symptoms of poisoning to sufficiently alert the crew when taken ill. Furthermore, at least two crew members were not present at that briefing.
- When the accommodation’s ventilation was stopped and the flaps closed, no consideration was given to the potential effects of this action or the additional risk posed by the fumigated cargo. Stopping the accommodation’s forced ventilation resulted in the positive pressure being lost in the accommodation and allowed the fumigant to enter.
- Periodic atmosphere monitoring was not conducted at the specified frequency. An increased periodic testing frequency may have identified the fumigant earlier. In addition, the carbide olfactory additive did not provide sufficient warning to the presence of the fumigant.
- The investigation found that once fumigant poisoning was identified, insufficient steps were taken to prevent the loss of life.
For more information on this incident email lossprevention@tindallriley.com.
THIS CASE STUDY IS DRAWN FROM THE INVESTIGATION REPORT PUBLISHED BY THE BAHAMAS MARITIME AUTHORITY.
THE PURPOSE OF THIS CASE STUDY IS TO SUPPORT AND ENCOURAGE REFLECTIVE LEARNING. THE DETAILS OF THE CASE STUDY MAY BE BASED ON, BUT NOT NECESSARILY IDENTICAL TO, FACTS RELATING TO AN ACTUAL INCIDENT. ANY LESSONS LEARNED OR COMMENTS ARE NOT INTENDED TO APPORTION BLAME ON THE INDIVIDUALS OR COMPANY INVOLVED. ANY SUGGESTED PRACTICES MAY NOT NECESSARILY BE THE ONLY WAY OF ADDRESSING THE LESSONS LEARNED, AND SHOULD ALWAYS BE SUBJECT TO THE REQUIREMENTS OF ANY APPLICABLE INTERNATIONAL OR NATIONAL REGULATIONS, AS WELL AS A COMPANY’S OWN PROCEDURES AND POLICIES.