
 English
EnglishThe second officer (2/O) on a general cargo ship was fatally injured when he was crushed between the ship’s gantry crane and a stack of cargo hold hatch covers (Figure 1) during post-cargo loading operations while alongside in port. The 2/O was attempting to pass between the hatch covers and the stationary crane on the main deck, when the chief officer (C/O) drove the crane aft, trapping and crushing the 2/O against the hatch covers.

Source: Marine Accident Investigation Branch (MAIB), © Crown copyright, 2020
WHAT HAPPENED?
The general cargo ship was berthed alongside and loading a cargo of cement. The 2/O came on watch shortly before midnight and at 0115 the cargo loading was competed. The 2/O remained on duty until 0540, when the C/O took over the watch again.
After 0830, the C/O started to lift and close the pontoon-type hatch covers using the ship’s rail-mounted gantry crane (Figure 2) and instructed the deck crew to commence cleaning cement dust from the hatch coamings. These tasks had to be completed before departure.

Source: Marine Accident Investigation Branch (MAIB), © Crown copyright, 2020
At about 0900, the agents informed the master that the pilot would be boarding at 1130, and not 1400, as the sailing time had been brought forward. The C/O therefore advised the master that all available hands would be needed to complete the cleaning and it was agreed that the 2/O would be called back.
The 2/O arrived on deck at about 0930 and commenced sweeping dust from the hatch cover landing surface on the starboard side of the aft cargo hold coaming. The 2/O was wearing overalls, safety shoes and a safety helmet. An able-bodied seamen (AB) was sweeping dust from the top of the aft hold’s hatch covers, while the other AB and the deck cadet were on the port side walkway cleaning the top of the forward hold coaming. The C/O remained on the gantry crane, moving various hatch covers. The deck cadet and two ABs were wearing face masks and eye protection, but the 2/O and C/O were not.
At 0942, the C/O moved a hatch cover to the forward end of the forward hold and lowered it into position and at 0943, he started to drive the gantry crane aft. At the same time, the 2/O finished sweeping and started to walk forward along the walkway. At 0944, the C/O stopped the crane just short of a stack of hatch covers at the forward end of the aft hold and started to raise the crane’s lifting bar. At 0944:10, the 2/O arrived at the forward end of the hatch cover stack and climbed onto the hatch coaming (Figure 3).
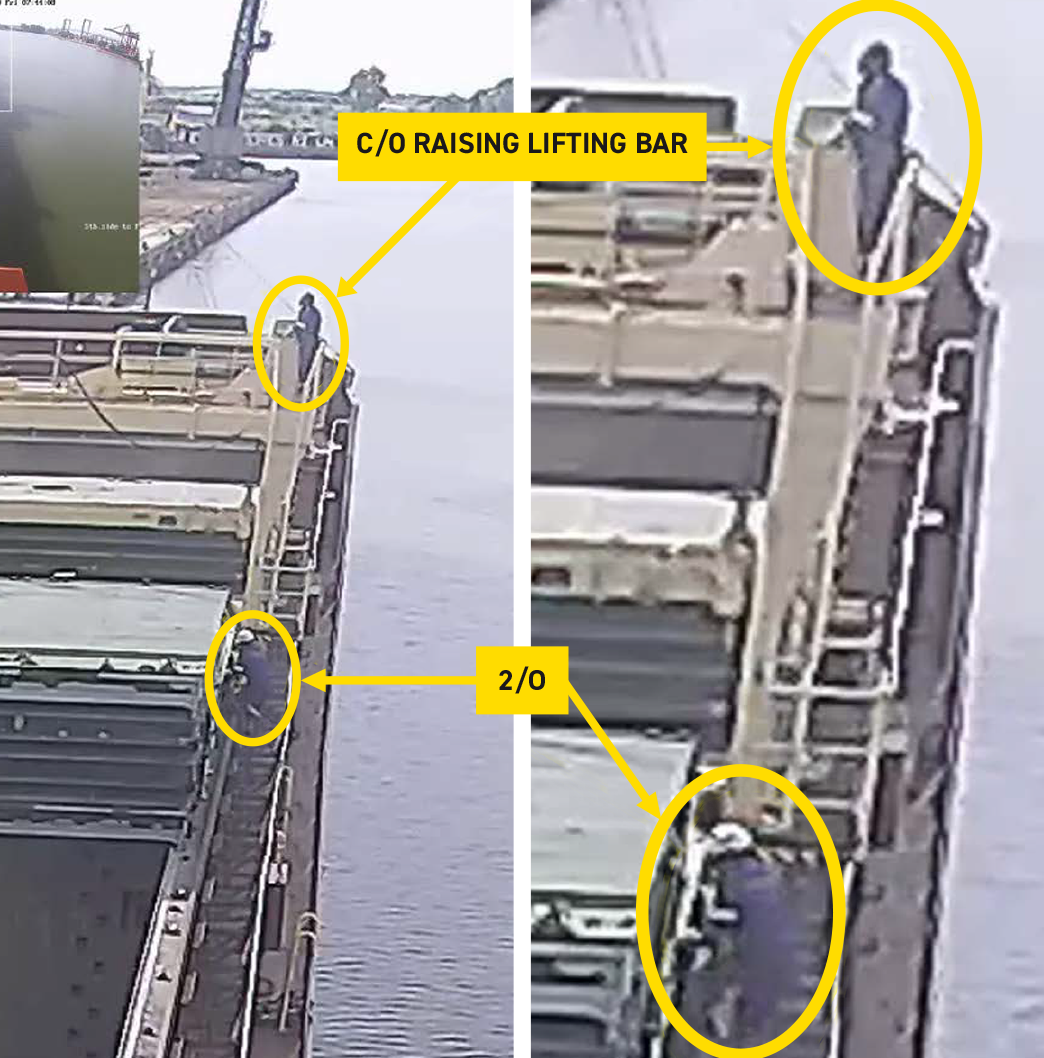
Source: Marine Accident Investigation Branch (MAIB), © Crown copyright, 2020
As he stepped towards the gap between the crane and the stacked hatch covers, the lifting bar cleared the hatch cover stack and the C/O drove the crane aft. The 2/O screamed as he was trapped and crushed between the hatch covers and the crane’s ladder access platform (Figure 1).
The crane stopped abruptly and the C/O immediately reversed the crane. As the crane moved forward, the 2/O was rolled between the crane’s ladder platform and the hatch covers and he then fell off the coaming onto the walkway below. As he fell, his head struck the guardrails on the side of the walkway. Reacting to the 2/O’s screams, the ABs and the deck cadet rushed to the scene. The 2/O soon lost consciousness and stopped breathing and the deck crew immediately commenced cardio-pulmonary resuscitation (CPR).
The C/O called the master on his radio and informed him that the 2/O had fallen and the master made his way to the scene within a minute, then called the ship’s agent, who alerted the emergency services. The master also called the Designated Person Ashore (DPA) and told him that the 2/O had fallen on deck.
At about 1005, two emergency medical teams arrived and the C/O told them that the 2/O had fallen from the coaming. Despite the efforts of the medical teams, the 2/O was declared deceased at 1100. The attending doctor told the master and C/O that the 2/O had possibly died as a result of a heart attack. However, the post mortem report concluded that the 2/O had experienced a violent accidental death, resulting from internal bleeding due to organ rupture. He had also suffered multiple fractures. The 2/O’s toxicology report stated that his blood alcohol content (BAC) was 117mg per 100ml. The incident occurred on the 2/O’s birthday.
The investigation noted that an emergency stop button was fitted to the crane platform, but the 2/O would have been unable to reach this while in the gap between the platform and covers.
Further details about the incident and the lessons learned are provided in the summary of the case study.
In addition, a presentation and reflective learning form have been prepared based on the incident as suggested training materials. These can be used by Members or their crew in any way they see fit to encourage reflection and gain the maximum learning from this incident: to consider why the incident happened; “what it means to me”, and to then relate the identified learning points to one’s own personal situation.
Finally, a Britannia commentary on the incident has been prepared which discusses the key points in more detail in order to help develop the reflective learning from the case study.
CASE STUDY MATERIAL
BSAFE INCIDENT CASE STUDY NO.7 – SUMMARY
BSAFE INCIDENT CASE STUDY NO.7 – REFLECTIVE LEARNING FORM
LESSONS LEARNED
The following lessons learned have been identified. These are based on the information available in the investigation report and are not intended to apportion blame on the individuals or company involved:
- The 2/O was crushed while he was trying to walk between the gantry crane and a stack of hold hatch covers when the C/O began to move the gantry crane aft at the same time.
- The 2/O was unaware that the C/O was about to move the crane, while the C/O was unaware that the 2/O was under the crane. Their situational awareness would have been enhanced if effective communications and proper control of the deck operations had been established.
- Before moving the crane, the C/O should have moved from the crane’s control position to check the walkways and ensure the area directly below was clear.
- The crane was fitted with a warning bell and flashing amber light, but these only operated while it was moving. A pre-movement warning device would have alerted the 2/O to the crane’s imminent movement.
- The crane’s deck level emergency stop buttons could only be operated from the walkways and could not be reached by the 2/O before and after he became trapped.
- The risk assessment and procedure for operating the gantry crane could have been clearer, but the incident would have been avoided if the stated safety controls had been implemented.
- The investigation concluded that the onboard safety culture was weak given that established safe systems of work were not being followed.
- The 2/O’s judgment and perception of risk were probably adversely affected by alcohol. The company’s drug and alcohol policy was not being effectively enforced.
- All known details of an incident should always be communicated to ensure the most appropriate medical treatment can be provided.
For more information on this incident email lossprevention@tindallriley.com
THIS CASE STUDY IS DRAWN FROM THE INVESTIGATION REPORT 18/2020 PUBLISHED BY THE MARINE ACCIDENT INVESTIGATION BRANCH (MAIB) (© Crown copyright, 2020)
THE PURPOSE OF THIS CASE STUDY IS TO SUPPORT AND ENCOURAGE REFLECTIVE LEARNING. THE DETAILS OF THE CASE STUDY MAY BE BASED ON, BUT NOT NECESSARILY IDENTICAL TO, FACTS RELATING TO AN ACTUAL INCIDENT. ANY LESSONS LEARNED OR COMMENTS ARE NOT INTENDED TO APPORTION BLAME ON THE INDIVIDUALS OR COMPANY INVOLVED. ANY SUGGESTED PRACTICES MAY NOT NECESSARILY BE THE ONLY WAY OF ADDRESSING THE LESSONS LEARNED, AND SHOULD ALWAYS BE SUBJECT TO THE REQUIREMENTS OF ANY APPLICABLE INTERNATIONAL OR NATIONAL REGULATIONS, AS WELL AS A COMPANY’S OWN PROCEDURES AND POLICIES.